
- You are here:
- Home »
- Blog »
- Joint Health / Pain »
- What to Do for An Angry IlioTibial Band? Stop Stretching It
What to Do for An Angry IlioTibial Band? Stop Stretching It
It doesn’t matter how you try to stretch the Iliotibial Band (ITB), what technique you use, or how hard you try, you can’t stretch it. It’s tensile strength is thousands of pounds per square inch which, when you stop and think about it, makes sense. Why would you want your fascia to easily deform with something like stretching or some type of manual treatment when its job is to hold things together?
The frustration in dealing with an angry ITB is summed up well in this email I received from a reader.
I stumbled upon your blog. Sitting here with a bag of frozen broccoli on an angry ITB. Ha. After a two year hiatus from running I have returned SLOWLY to walking, swimming and some running. My ITB flared up in the past and lay dormant all this time- waiting to reclaim its hold on any plans of race day glory. Im 37 years old and feel like the clock is ticking too fast.
I consider myself an expert on the vast blogs and internet approaches to treating ITB. I have done every “ITB…marathon training..physical therapy… running” web search. I have read it all!. You are one of the FEW people I have read that touts the impracticality of stretching a brick. Your argument made a lot of sense.
I found your take very interesting. I’m 37, fit and interested in a conservative approach to learning HOW to address the ITB problem. I am overly flexible, and probably lack strength. I have had some success with PT- but everyone says stretch it, stretch it, stretch it. I wound up with a nasty hip bursitis (which began my running hiatus).
Do you have any tips on HOW to treat ITB generally speaking. (I know you cannot treat people over internet). I just mean…do you suggest massage, roller or specific hip strengthening-all things equal.
Sorry if I rambled. I am a frustrated wanna be athlete.
Thank you, in advance, for any info you might share.
Sincerely,
J
Conventional wisdom, as J discovered, is to stretch an irritated ITB…even though you can’t.
Treatment of ITB Syndrome: Fundamentals
There are three main components of any musculoskeletal injury: biomechanics, tissue injury, and attitude. What the reader has bumped into is that most approaches for this problem come at it from one of the components, usually biomechanical (orthotics, stretching, etc), and leave out the other two. So, if you actually have tissue damage in the ITB, which is entirely possible, and you correct the biomechanics, the tissue is still weak. So, when you resume loading it, as in running, symptoms return.
Make sure you really have ITB Syndrome and not degenerative joint disease / chondromalacia of the knee. Fluid from inside the joint can find its way under the the ITB which then increases the pressure between the ITB and the bursa. Other signs and symptoms of a joint problem (DJD or Chondromalacia) include pain, aching, stiffness, a sense of fullness in the knee. You should also have a positive Noble’s Test – a test for IT Band Syndrome (pressure applied to the lateral condyle of your femur while flexing and extending your knee through 30 degrees of motion).
Biomechanics
- People with ITB Syndrome tend to have a high medial arch of the foot and impaired control of the rear foot. Your orthotics should correct for that, if you have it, and not for the more common “flat foot” found in the general population.
- Make sure you have adequate dorsiflexion of the ankle as inflexibility is associated with ITB Syndrome. If you lack motion, find out if it’s from tightness or structural limitations (you’ll need a therapist to help you).
- Check your hip strength since weakness of the gluteus medius is common in ITB Syndrome. Stand on a step with one leg off the step allowing the hip to drop. Hike your hip up without rotating the pelvis right or left. You should be able to bring the top of the pelvis well above the horizontal and be able to do this at least 10 times. Check both sides. Usually, the side with symptoms will fatigue sooner and / or you will not be able to keep the pelvis from rotating. I also use a digital muscle tester to test hip strength using other motions which provides an exact measurement of strength and I can compare this to the other side as well as to a ratio of strength to body weight. Either case, if your hip muscles are too weak, you’re not ready to run.
- Check your single leg squat strength. Stand in front of a chair on one leg with the back of your leg just in front of the chair. Hold your other leg off the ground in front of you. Squat down until your knee reaches a 70 degree angle and then stand up. Watch the pattern of motion of your leg. Your knee, as you look down on it, should travel in a reasonably straight line. If not, if it tends to wobble in and out, your hip muscles and leg muscles are weak. You should not run until you can squat up and down at least 30 times with good control.
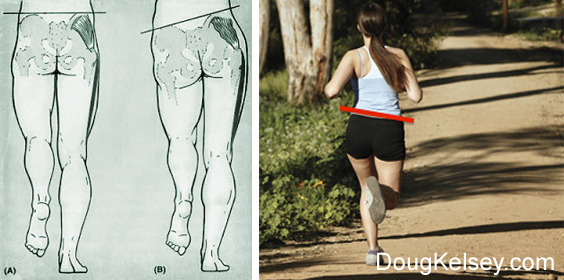
- Have a friend video you running from behind and then look at the angle your hips make with the horizon when your foot hits the ground. There should be little to no “drop” of the hip. In this image, you can see the drop I’m referring to. When your hip drops, the femur (thigh bone) will rotate inward which then increases the pressure of the ITB against the leg.
Address the Tissue Injury
Assuming there is one which in most cases is not an inflammatory disorder (as in tendonitis) but a tendonosis (and if you actually have a joint disorder, that’s another story)…
The treatment of tendonosis always involves discomfort. The exercise needs to stress the tissue. I usually use squats – single leg – at a load level that produces some discomfort in the leg between 20-30 repetitions and aim for 30 repetitions. I often use squats in supine (lying on your back) and in a sidelying position on a Total Gym or Total Trainer since almost everyone I’ve seen with ITB Syndrome fails the hip and leg strength tests and has to exercise with less than full body weight. Perform 3 sets resting about 1 minute between the sets. This yields 180 repetitions of load and depending on your body weight, could be between 6000 and 10,000 lbs of load.
People often get anxious about pain during the exercise. Tendonosis pain generally won’t hang around long after the exercise and the degree of pain should be mild to moderate.
As your leg gains strength, I usually add hopping on the Total Gym / Total Trainer until you pass the hip and leg strength tests and then begin some limited hopping full body weight. The hopping prepares your leg for running.
I use sidelying hip abduction drills (some call these hip or leg lifts). While on your side with the bottom hip and knee bent, align the upper leg such that it forms a straight line with your trunk. Lift the leg up and down like a pump handle keeping it straight.
As you fatigue, your leg will want to drift forward. If you cannot keep the leg in the proper position, stop. This exercise will fatigue the hip muscles considerably and stress the iliotibial band.
I also use standing hip abduction drills. Standing on the symptomatic side, I attach a pulley to just above the ankle of the other leg (you could also try an elastic band). Now, bend the weight bearing knee about 20 degrees. This activates the hip muscles. Move the opposite leg away from the body and then back. Repeat this 30 times, 3 sets with a minute of rest in between.
Address Inflexibility and Pain
I use a foam roller under the involved side. Lying on top of it, just roll your leg back and forth, up and down. It doesn’t matter which pattern you use. It will likely hurt. If a tennis ball feels better, use it. This procedure often reduces pain and improves flexibility through reflexive relaxation of the hip muscles.
I use Capsaicin as a topical agent over the region of pain to reduce symptoms. You can find Capsaicin in most any grocery or drug store.
Address Attitude
Your attitude is reflected in how well you pay attention to your symptoms and the choices you make. A very difficult thing to do, for just about everyone, is to accept your current state of abilities and work from that level. If you find yourself refusing to stop running, for example, despite symptoms that force you to stop or cause you to modify your running, you have an attitude problem. No amount of physical treatment will work in the presence of an attitude that runs on denial.